Introduction toPelvic UltrasoundPart 1: Benign Ovarian and Adnexal Cystic Lesions
September, 2012
Mindy M. Horrow, MD, FACR, FSRU
Director of Body Imaging
Einstein Medical Center
Professor of Radiology
Jefferson Medical College
Types of US Imaging
•Transabdominal
•Transvaginal
•Translabial
•Transrectal
Higher frequency, better resolution
Lower frequency, better penetration
AEMC Policy: Do not have women arrive with distended bladder. Ifnever previously scanned, do transabdominal sag and transverseimages. Decide on full TA and/or TV scan.
Trans vaginal imaging of uterus in different positions


Initial trans-abdominal imaging, then trans-vaginal

US and CT after C-section
Difficult scanning by TA and TV methods
Uterus in Adulthood
•Nulliparous uterus with maximal dimensions of 8 x5 x 4 cm, increasing with multiparity
•Atrophies after menopause. After age 65, rangesfrom 3.5 to 6.5 cm in length and 1.2 to 1.8 cm AP
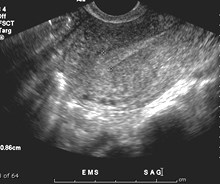
•Endometrium varies during menstrual cycle.Endometrial cavity consists of thin echogenic lineresulting from interface between opposingsurfaces of endometrium.


EMS duringmenses, blood inendometrial canal
Earlyproliferativephase EMS
N.B. Endometrial stripe measured as double thickness in sagittal view
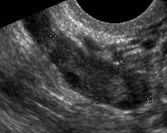
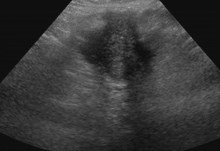
Pre-Ovulatory Study
Dominant follicle, trilayered endometrium


Secretory phase endometrium
Endometrium
•Menses: thin echogenic line
•Proliferative phase: hypoechoic measuring 4-8mm
•Periovulatory phase: triple layer 6-10 mm
•Secretory phase: hypoechoic measuring 7-14 mm(secondary to mucus and glycogen in glands andinterfaces from tortuous vessels)
•Postmenopausal phase: if bleeding < 4-5 mmconsidered normal, no bleeding up to 6-8 mmconsidered normal
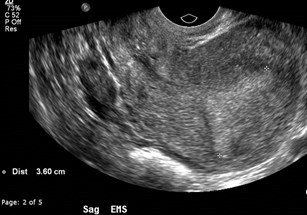

Is endometrium too thick?
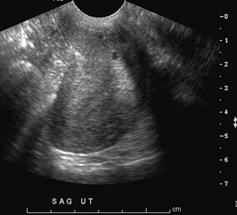
Must measure endometrium in true sagittal image

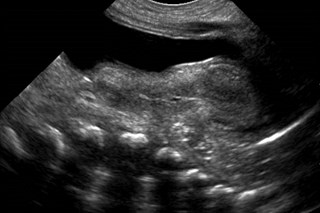
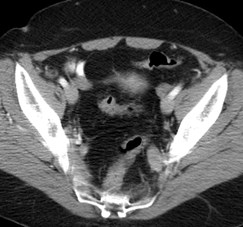
64 year old diabetic
Peripheral vascular calcifications: a normalaging process accelerated in diabetics
(Monkeberg’s sclerosis)

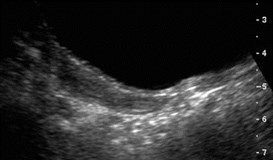
Elderly, incontinent patient with postmenopausal bleeding
Transrectal US: Atrophic EMS with fluid, cervical stenosis


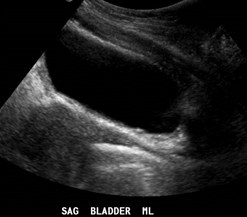
Post void
Retrograde filling of vagina
Tampon in Vagina
Patient gives history of hysterectomy

Transvaginal view in transverse
Supracervical Hysterectomy
Ovary
•Variable position, sometimes requiring both TA and TVimaging, long axis parallels internal iliac vessels
•Appearance changes with age and phase of menstrualcycle
•Early proliferative: multiple follicles begin to increase insize from FSH and LH until day 8-9
•One follicle becomes dominant, reaching 2.0 – 2.5 cmby ovulation, others become atretic
•After ovulation, corpus luteum develops as hypo orisoechoic structure, involuting before menstruation
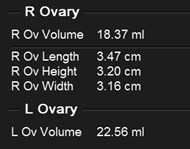
Ovarian Volume
•0.523 x length x width x height
•Upper limit of normal in first 3 months 2.7 cc, 4 – 12months 1.7 cc remaining stable until age 5
•Ovarian volume gradually increases up to menarchewhen mean volume is 4.2 cc
•Small follicles common in neonatal and premenarchalovaries.
•Adult: mean volume 9.8 5.8 cc
•Ovary atrophies after menopause, with most folliclesdisappearing in first few years. Mean volume 1.2 – 5.8cc. Greater than 8.0 cc considered abnormal.
Management of Asymptomatic Ovarian and Other Adnexal Cysts Imagedat US: Society of Radiologists in Ultrasound Consensus ConferenceStatement1
Abstract
The Society of Radiologists in Ultrasound convened a panel of specialists fromgynecology, radiology, and pathology to arrive at a consensus regarding themanagement of ovarian and other adnexal cysts imaged sonographically inasymptomatic women. The panel met in Chicago, Ill, on October 27–28, 2009, anddrafted this consensus statement. The recommendations in this statement arebased on analysis of current literature and common practice strategies, and arethought to represent a reasonable approach to asymptomatic ovarian and otheradnexal cysts imaged at ultrasonography.
Deborah Levine, Douglas L. Brown, Rochelle F. Andreotti, Beryl Benacerraf, Carol B. Benson, Wendy RBrewster, Beverly Coleman, Paul DePriest, Peter M. Doubilet, Steven R. Goldstein, Ulrike M. Hamper,Jonathan L. Hecht, Mindy Horrow, ye-Chun Hur, Mary Marnach, Maitray D. Patel, Lawrence D. Platt,,Elizabeth Puscheck, Rebecca Smith-Bindman


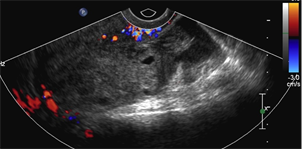
Dominant follicle ruptures during study:OVULATION
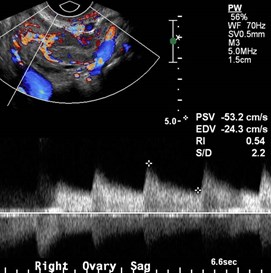
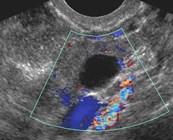
Corpus luteum
“Tennis racket blood flow”
Normal Ovary
•During menstrual years a simple cyst up to 3cm isconsidered normal
•During menstrual years a corpus luteum with typicalflow and an appearance ranging from cystic to solid isconsidered normal
•After menopause, folliculogenesis stops. Howeversmall < 1cm simple cysts are common, in up to 21%


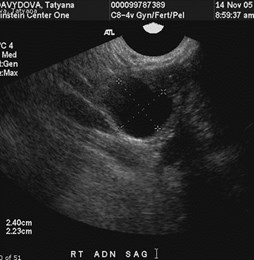
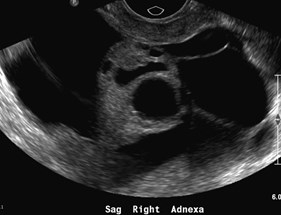
RLQ pain in 22 year old
Right ovary with simple cyst and leakinghemorrhagic corpus luteum

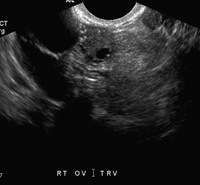
Echogenic foci in ovaries
Two different patients
Echogenic ovarian foci
•Specular reflectors from tiny unresolved cysts
•Hemosiderin
•Calcification
•Superficial epithelial inclusion cysts andassociated psammomatous calcifications
Muradali.Radiology 2002;224:429
Brown.. JUM 2004;23:307
Kupfer. AJR 1998;171:483
Menopause
•Defined as amenorrhea for one year after final menses
•In Western countries average age is 51-53 years withwide variation
•Early menopause: 1-5 years post menses
•Late menopause: > 5 years post menses
•Ovulatory cycles are infrequent in menopause, but mayoccur during early menopause


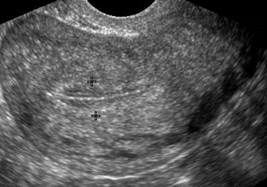
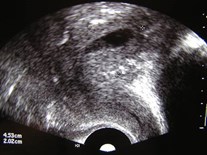
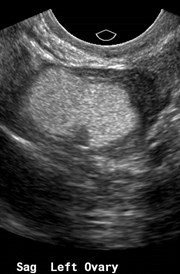
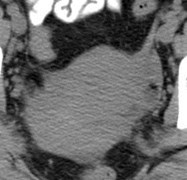
Normal ovaries, 4 years postmenopausal
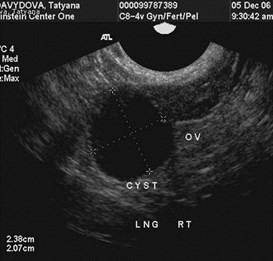
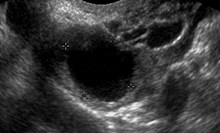
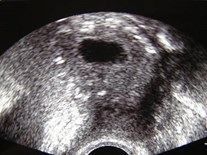
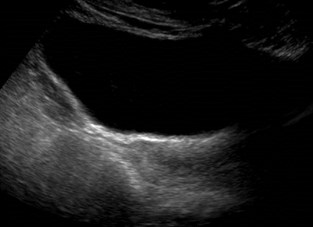
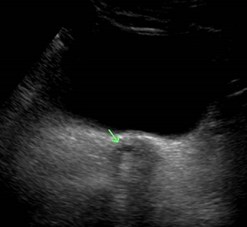
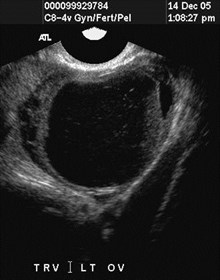
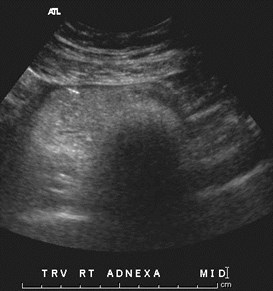
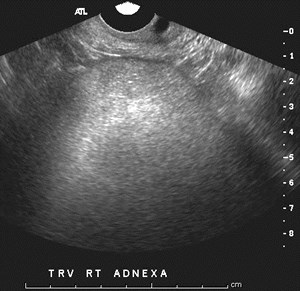
Post Menopausal Patient
Stable, simple ovarian cyst
Management of Cysts in Post MenopausalWomen
•Cysts ≤ 1cm do not require follow up
•Simple cysts > 1cm and ≤ 7cm are highly likely to bebenign. At least one yearly follow up recommended.Further follow up unclear, though more likely at largerend of size range.
•Cysts > 7cm may be difficult to completely evaluatesonographically. Consider MR and/or surgical removal.
Management of Cysts in Pre MenopausalWomen
•Cysts ≤ 3cm are physiologic and description in reportup to individual
•Cysts > 3cm and ≤ 5cm almost certainly benign and donot require follow up
•Cysts > 5 cm and ≤ 7cm almost certainly benign andmay be followed at 12 months
•Cysts > 7 cm may be difficult to completely evaluatesonographically. MR should be considered.


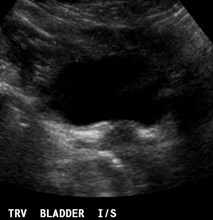
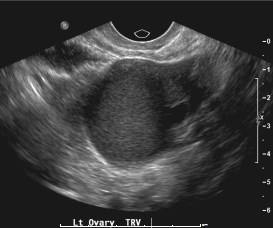
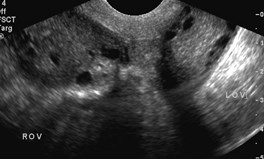
TRV LOV
TRV ROV
Newborn Pelvis

TRV ROV
TRV LOV
Normal 4 year old pelvis

Normal 10 year old pelvis

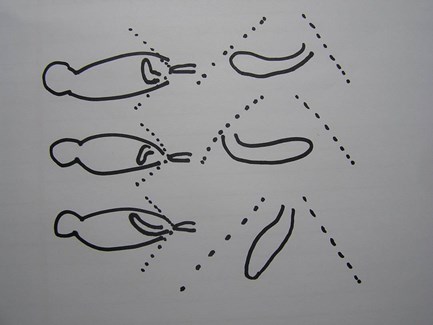
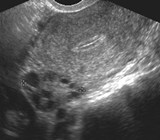
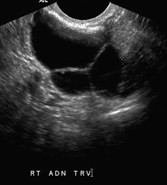
Normal Fallopian tube outlined by blood fromruptured hemorrhagic cyst, small amounts simplefree fluid are normal throughout cycle
Normal Fallopian Tubes




Two different patients with same diagnosis
Hydatid of Morgagni (paratubal cyst)
Adnexal Cysts
•Hydatid of Morgagni: Common remnants of theMullerian duct located below the fallopian tube near thefimbria
•If detected sonographically, appear as a simple cysts
•Clinically insignificant and rarely cause symptomsunless they undergo torsion and infarction
•Para ovarian cysts also common
•Recommendation: No real literature on follow up ofthese lesions. Our experience is that they remainstable. May apply ovarian cyst recommendations.
Common OvarianLesions
Hemorrhagic Cyst: resolves





Other Hemorrhagic Cysts
With Rupture
Hemorrhagic Cyst
•Due to expanding hemorrhage in corpus luteumor other functional cyst
•Sonographic features that allow confidentdiagnosis: mass with reticular pattern of internalechoes (fishnet, cobweb, spiderweb, lacy,generally due to fibrin strands) and/or solidappearing area with concave margins, no internalflow and usually circumferential flow in wall.Wall thickness is variable.
•Usually resolve within 8 weeks.
Study on 5-26

Normal left ovary withsmall follicles
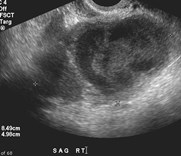
Normal right ovary withhemorrhagic corpusluteum
Normal uterus withsecretory phaseendometrium

Repeat exam 6-8

Normal left ovary withdeveloping dominantfollicle
Normal right ovary withmultiple small follicles andresolution of previouscorpus luteum
Normal proliferativeendometrium
Uterus and ovaries should correlate with phase ofmenstrual cycle
Hemorrhagic Cyst: recommendation
•Typical hemorrhagic cyst ≤ 3cm, not necessary toreport or follow up
•Typical hemorrhagic cyst > 3cm and ≤ 5cm should bereported, but does not require follow up
•Typical hemorrhagic cyst ≥ 5cm should have shortterm (6-12 week) follow up
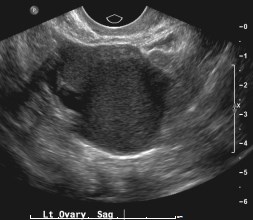
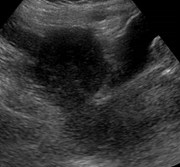
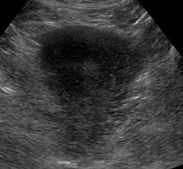
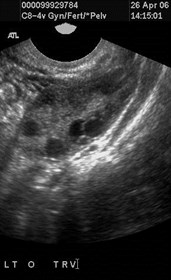
Non-pregnant, left pelvic pain
Endometrioma

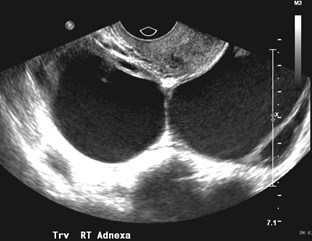
Bilateral endometriomas
Endometriosis
•Diffuse form: more common, multiple endometrialimplants, hormonally responsive, rarely diagnosedsonographically, symptoms include dysmenorrhea,dyspareunia, infertility
•Localized form: discreet endometrioma, usuallyasymptomatic, often multiple
•Most commonly occurs in ovary, fallopian tube, broadligament, posterior cul-de-sac, but can be almostanywhere.
Endometriosis
•Endometrioma is most readily diagnosed form onUS and MR
•US: cystic lesion with fine low level echoes, maybe multilocular with thin and thick septations.Round echogenic foci are caused by clotformation or cholesterol deposits, occasional fluid-fluid level.
•MR: cystic mass with high signal on T1 and lossof signal on T2
Endometrioma:recommendations
•Classic lesions should have some follow up if notsurgically removed.
•Atypical lesions that may overlap hemorrhagiccyst should have shorter interval follow up in 6 to12 weeks
•Malignancy in 1%, uncommon in lesions < 6cmand more common if > 9cm in women older than45 years. Latency period several years. Look forrapid growth or development of flow in solidcomponent.




6 different lesions, same diagnosis
Dermoids = Mature Cystic Teratomas

Bilateral Dermoids
TV TA
Teratoma: all dermoid plug, no fluid


Teratoma with multiple fat containingcomponents


Post menopausal woman
Bilateral Dermoids


Dermoid with floating fatty locules
Dermoids: recommendations
•With classic appearance: focal or diffuse hyperechoiccomponents, echogenic lines and dots, acousticshadowing, no flow on Doppler, floating sphericalstructures (rare), no confirmatory imaging necessary.
•If not surgically removed, follow up ultrasound in oneyear.
•Malignant degeneration in 0.17 to 2%, usually women >50 years and large (> 10cm) lesions. Look for growth,flow in solid component, spread.


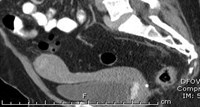
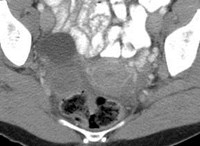
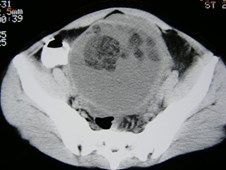
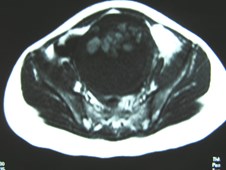
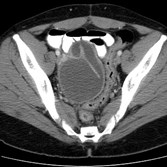
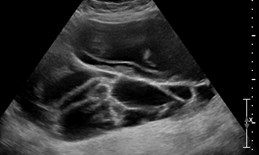
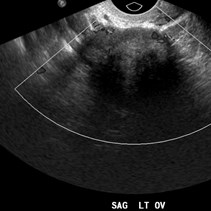
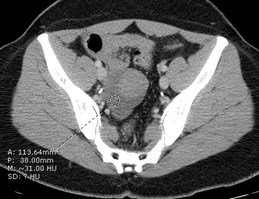
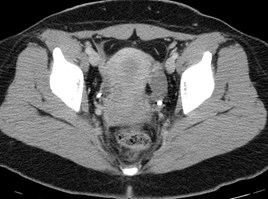
ER CT for pain in a
36 year old

Peritoneal Inclusion Cyst
Peritoneal Inclusion Cyst
•Fluid produced by ovaries accumulates withinadhesions, entrapping ovaries, resulting in large cysticadnexal mass.
•History prior surgery, trauma, PID, endometriosis
•US: multiloculated cystic masses partially or completelysurrounding intact ovary. May have septations or lowlevel echoes. Follow contour of adjacent organs orperitoneal cavity.
•Recommendations: If classic features no furtherimaging or follow up ultrasound. Further evaluation ifatypical.

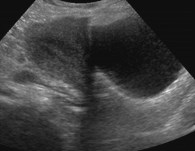
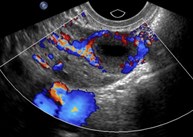
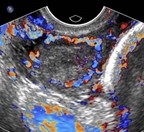
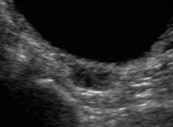
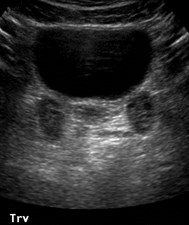
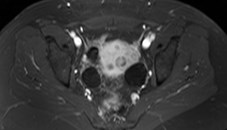
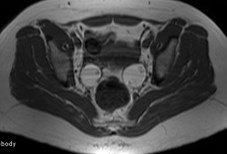
Post menopausal woman sent for evaluation ofovarian neoplasm
Hydrosalpinx


Hydrosalpinx: 2 examples
Hydrosalpinx
•US: tubular fluid filled structure with short roundprojections (“beads on a string” representingendosalpingeal folds, or “waist sign” reperesentingindentations on opposite sides, often have incompletesepti
•Cine clips or 3-dimensional imaging may be helpful toprove tubular nature
•Should be separate from ipsilateral ovary
•Recommendation: no further imaging if classicappearance, no set interval US follow up


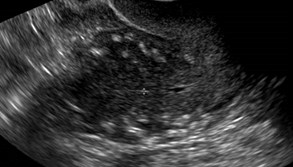
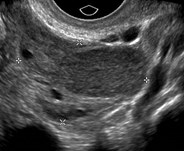
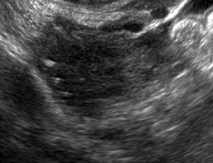
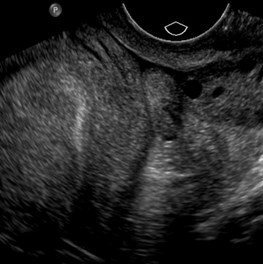
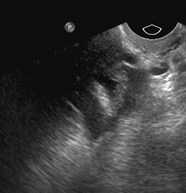
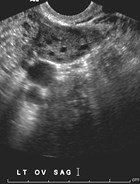
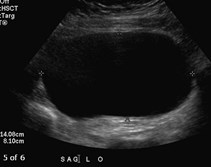
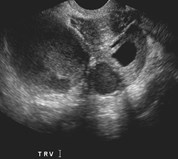
21 year old with irregular menses
Polycystic Ovarian Syndrome
•The European Society for Human Reproduction and Embryology(ESHRE) and the American Society for Reproductive Medicine(ASRM) recommended that at least 2 of the following 3 featuresare required for PCOS to be diagnosed
–Oligo-ovulation or anovulation manifested as oligomenorrhea oramenorrhea
–Hyperandrogenism (clinical evidence of androgen excess) orhyperandrogenemia (biochemical evidence of androgen excess)
•Polycystic ovaries (as defined on ultrasonography)
•Polycystic ovaries are defined as 12 or more follicles in at least 1ovary measuring 2-9 mm in diameter or a total ovarian volumeof >10 cm3.


48 year old
Serous Cystadenoma

Mucinous Cystadenoma

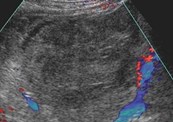
46 year old woman
Ovarian Fibroma
29 year old ER CT for acute right sided pain,possible appendicitis


Ovarian Torsion
Pelvic Pain
Right TOA and Left Pyosalpinx
The End

Lassen National Park, California 7-2012


Post menopausal woman with breast cancer

2008 2012
Metastatic breast cancer to ovaries